Soft Cast Layering Technique: Tension, Overlap, and Molding for Semi-Rigid Support
The quality of a semi-rigid soft cast depends primarily on layering technique. Even a high-grade medical fiberglass cast bandage can fail if applied with excessive tension, uneven overlap, or poor molding—resulting in either painful over-rigidity or inadequate support. This practical guide breaks down the three pillars of a correct semi-rigid result: tension, overlap, and molding.

Pillar 1: Tension control for a standard semi-rigid result
Soft cast tension must be controlled and consistent. Too much tension causes focal pressure, pain, blisters, and potential circulation issues. Too little tension results in looseness, unwanted motion, and poor stability. The goal is to restrict risky motion without creating neurovascular symptoms.
- Key rule: Pull until flat and wrinkle-free—not tight and glossy.
- Keep it consistent: Each turn should feel similar to the previous one.
- Reduce tension on bony prominences: malleoli, styloid processes, ulnar head, navicular zones.
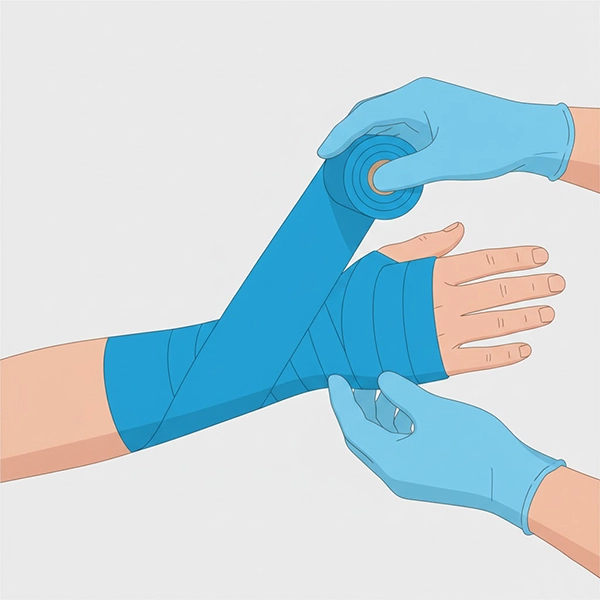
Pillar 2: Overlap precision—why 30–50%?
Standard overlap for most soft cast applications is 30–50%. This distributes forces evenly and avoids sharp ridges or pressure lines. Less than 30% can create weak points; excessive overlap increases unnecessary thickness and stiffness.
- Cylindrical segments (forearm/calf): 40–50% overlap often works best.
- High contour areas (wrist/ankle): 30–40% plus accurate molding.
- Consistency matters: uneven overlap creates asymmetric thickness.
Pillar 3: Molding—turning wrapping into true cast construction
Many failures happen when the cast is only wrapped, not molded. Molding means shaping the cast with open palms and controlled pressure to lock in functional joint alignment. In semi-rigid casting, molding creates stability without adding layers.
- Avoid fingertips: fingertip pressure creates hotspots and sores.
- Use the “golden window”: typically 30–90 seconds after wrapping (depends on water temperature and brand).
- Functional positioning: ankle neutral, wrist functional extension, thumb in appropriate abduction.
Timing management: water activation and working speed
- Lukewarm water: best for predictable working time.
- Short dunk: usually 2–5 seconds is enough.
- Gentle squeeze: avoid aggressive wringing that disturbs resin distribution.
Common layering errors and fixes
- Pressure lines: uneven overlap or fingertip molding → uniform overlap + palm molding
- Loose cast: low tension or insufficient roll length → improve tension control and sizing
- Over-rigidity: excessive overlap/layers → reduce thickness and prioritize molding
- Sharp edges: poor termination → soft edge finishing and reinforcement

Quick checklist for clinic staff
- Uniform 30–50% overlap throughout
- Controlled tension: wrinkle-free, not overly tight
- Palm molding, not fingertip pressure
- Maintain functional joint positioning
- Check CSM (color/sensation/motion) after application
- Educate patient on care and red flags
Conclusion
A high-quality semi-rigid soft cast is built on three skills: proper tension, precise overlap, and professional molding. When these principles are applied, maximum stability and comfort can be achieved with minimal thickness—improving both outcomes and patient experience.
Call to Action
For staff training, technique standardization, or selecting the right casting materials for your clinic:
Contact & Clinical Consultation