Athletes and Soft Cast: Gradual Return to Training and Competition
For athletes, “return to training” is not a single decision—it is a staged pathway that must protect healing tissues while maintaining performance capacity. In many mild-to-moderate injuries (e.g., Grade I–II ankle sprains, wrist ligament strains, selected stable thumb injuries), a soft cast as a semi-rigid immobilizer can provide a smart balance between support and controlled mobility. This guide outlines practical return-to-sport (RTP) principles and how soft casting fits into a phase-based plan.

Why soft casts are attractive for athletes
Athletes typically face two competing priorities: protect the injury and preserve fitness. Rigid casts can promote stiffness, proprioceptive loss, and deconditioning. Soft casts, when appropriately indicated, may allow earlier controlled activity while limiting high-risk motions—provided protocols and adherence are in place.
Injuries that benefit most
- Grade I–II ankle sprains (no clear instability or associated fracture)
- Mild–moderate wrist ligament strains and overuse soft-tissue injuries
- Stable thumb injuries using semi-rigid spica technique
- Step-down phase after acute splinting or after rigid cast removal
When a soft cast is not ideal
- Unstable or displaced fractures
- Grade III sprains or clear joint instability
- Neurovascular red flags (progressive pain, numbness, pallor, color changes)
- High likelihood of non-adherence to restrictions
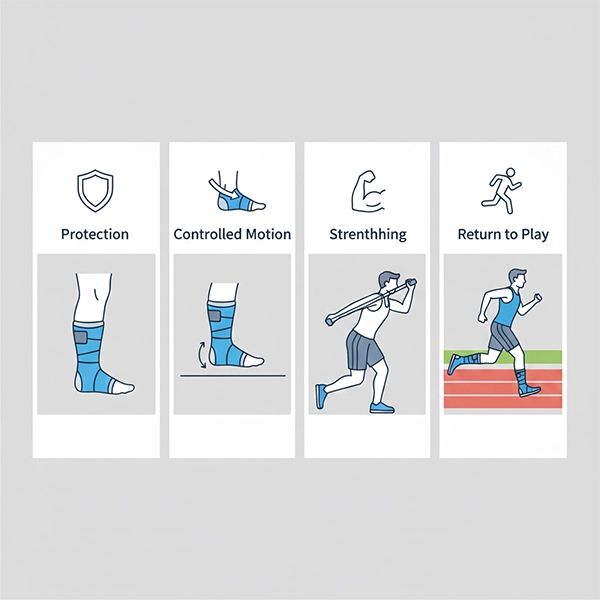
Return-to-sport (RTP) with soft cast: a phase-based model
In sports medicine, RTP is typically managed through phases. A soft cast can support early and mid phases, but it never replaces functional testing and clinical reassessment.
Phase 1: protection and symptom control (Day 0 to 3–5)
- Reduce pain/swelling: relative rest, ice, compression, elevation
- Short-term splinting may be used until swelling settles
- Education: rushing back too early increases recurrence risk
Phase 2: semi-rigid immobilization and controlled motion (≈ Day 3 to 14)
Soft cast limits high-risk movements (e.g., excessive inversion in ankle sprains) while enabling safe, low-load work.
- Allowed: pain-free ROM, isometrics, light balance drills in a safe environment
- Avoid: jumping, rapid cuts, explosive change-of-direction, contact drills
- Daily monitoring: skin/edges, tingling, escalating pain, swelling patterns
Phase 3: strengthening and sport-specific pattern restoration (Week 2 to 4)
As symptoms settle, the soft cast may be used as supportive protection or transitioned to bracing/taping. Progression should be based on function, not only pain reduction.
- Targeted strength (peroneals for ankle, forearm stabilizers for wrist)
- Proprioception and dynamic balance training
- Low-risk technical drills (no contact, no high-risk cutting)
Phase 4: controlled return to team training and competition (Week 3 to 6+)
Return-to-competition decisions should rely on practical criteria: near-symmetry strength, adequate ROM, successful balance tests, and pain-free sport-specific skills without fear of movement.
- Gradual increase in training intensity and volume
- Ongoing support: brace, taping, or in specific cases soft-cast support per clinician
- Risk management: recovery, sleep, nutrition, and avoiding rushed progression
Practical clinic tips for athletic soft casting
- Joint position: ankle neutral; wrist functional extension; thumb in appropriate abduction (spica)
- Layup: 30–50% overlap with even tension; reinforce pressure points
- Edge finishing: soften edges to reduce blisters/dermatitis
- Care education: keep dry, no objects under cast, monitor red flags
- Follow-up: review at 3–7 days to reassess swelling and fit
Common mistakes
- Explosive drills before proprioception and balance are restored
- Ignoring night pain, numbness, or color changes
- Using a soft cast as a “permission slip” to compete without functional testing
- Repeated wetting leading to skin irritation

Conclusion
For athletes, a soft cast is best when the injury is stable and the goal is adequate support with controlled mobility. With a structured phase-based RTP plan, clinicians can reduce recurrence while enabling a safer, faster return to training and competition. Final clearance should be guided by clinical reassessment and functional testing—not pain relief alone.
Call to Action
For clinical consultation on athlete immobilization strategies and RTP protocol design:
Contact & Clinical Consultation